Colorectal cancer (CRC) is one of the most common specimens GI pathologists get. Colorectal cancer causes a significant number of deaths per year, and young-onset CRC is increasing for unknown reasons. Pathologists play a critical role in the prevention of colorectal cancer (surveillance colonoscopies, identification of syndromic CRC, etc.), but they can also drastically impact the prognosis and management of CRC.
These were all reasons Dr. Rish K. Pai, MD, PhD, Pathologist at the Mayo Clinic, wanted to focus on CRC and further investigate how AI can augment the pathologists’ role and help guide oncologic decision-making. This article is based on Dr. Pai’s presentation at Aiforia’s webinar “Using prognostic AI models in pathology: case colorectal cancer.”
Watch the webinar recording here →
Stage II and stage III colorectal cancer
Stage II CRC is deeply invasive but hasn’t spread to lymph nodes. Stage III has spread to lymph nodes but not yet to other parts of the body (distant metastasis). These are the key stages at which the oncologist relies on the pathologist’s report for guidance, and thus, the stages Dr. Pai wanted to focus on in developing the AI model.
Stage II colorectal cancer
Stage II CRC patients can be divided into three sub-groups based on current American Society of Clinical Oncology (ASCO) guidelines:
- Low-risk group → No chemotherapy; observation.
- Intermediate risk group → Adjuvant chemotherapy may be offered to reduce the risk of recurrence.
- High-risk group → Should be offered adjuvant chemotherapy.
The stage II ASCO scheme risk stratifies patients based on their risk of recurrence. The oncologist then uses that information to decide whether to give chemotherapy.
Stage III colorectal cancer
The important decision in stage III CRC cases is not whether to give chemotherapy but how long to give it. For patients at a high risk of recurrence (T4 and/or N2), adjuvant chemotherapy should be offered for a duration of six months. For patients at low risk of recurrence (T1, T2, or T3 and N1), either six months of adjuvant chemotherapy or a shorter duration of three months may be offered based on a potential reduction in adverse events and no significant difference in disease-free survival with the three-month regimen.
- Low-risk stage III → Three-month chemotherapy
- High-risk stage III → Six-month chemotherapy
The risk level is currently decided based on the pT4 and/or pN2 categories. However, other important features might be beneficial.
Improving prediction of recurrence with AI
The decision whether to give chemotherapy in stages II and III is based on pathologic features that are diagnostically challenging, features that pathologists disagree on. Furthermore, while pathologists might believe some features are more important, oncologists do not use those in their evaluation. The current list of all the prognostic and predictive factors of CRC has too many features for oncologists to examine.
“If there is a way to integrate a lot of these features into one prognostic model, that can be more powerful. I think this is a perfect example of where AI can be useful.” – Dr. Rish K. Pai, the Mayo Clinic
Dr. Pai wanted to combine the current ASCO risk scheme with the AI model to provide a better tool for oncologists to risk stratify tumors. His hypothesis was:
Improved quantification of known features can improve the prediction of recurrence. The assumption is that we already know what drives prognosis in CRC; the problem is measuring those features.
Dr. Pai started developing the model with Aiforia®️ Create, the most versatile tool for creating, customizing, and validating deep learning AI models for image analysis, both in research and clinical settings.
Developing the QuantCRC model
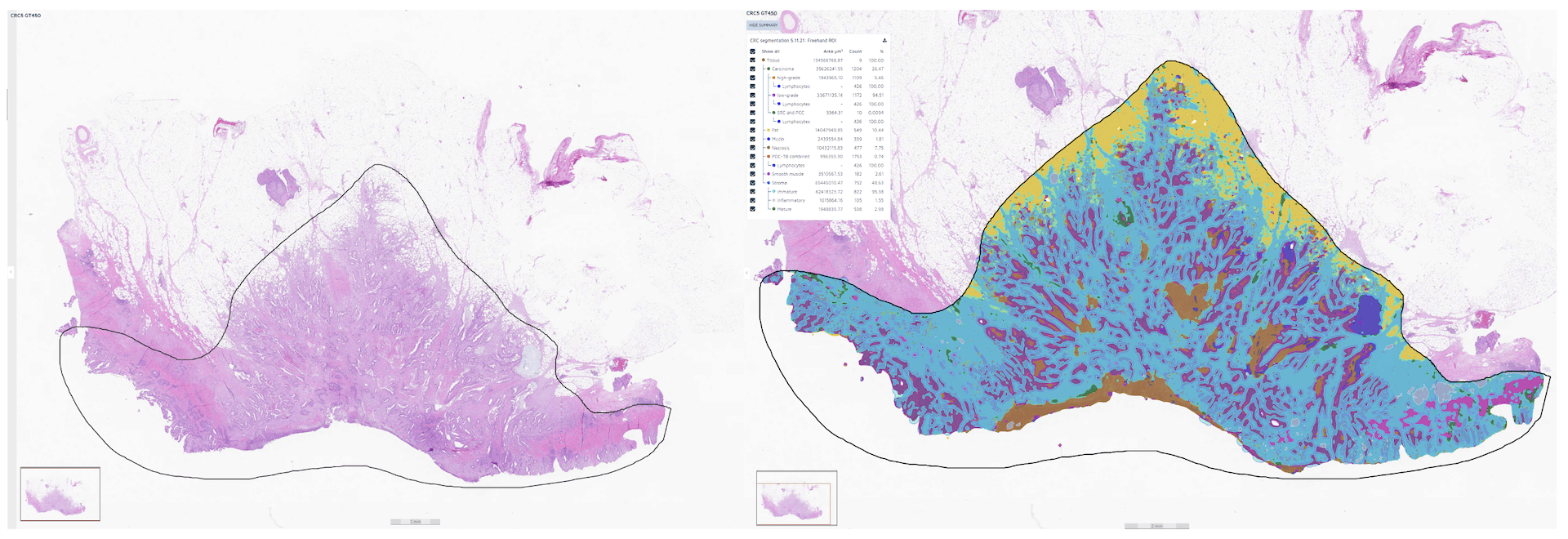
The training process of the new AI model, QuantCRC, included 24,157 annotations and 5,209 training sessions. The H&Es were from multiple labs, which ensured a lot of variability. All the images were scanned at 40X and 20X using Aperio GT450 and AT2.
Dr. Pai predefined what he wanted the model to learn. He chose the following CRC pathologic features:
- Tumor grade
- Mucin
- Necrosis
- Tumor budding
- Poorly differentiated clusters
- Stroma subtypes: Immature, inflammatory stroma, and mature stroma
- Tumor-infiltrating lymphocytes
From this data, Dr. Pai chose 15 features for the final AI model.
The QuantCRC model
After that, QuantCRC was applied to a large cohort of 7684 H&E slides: 607 were excluded, and 7077 were analyzed further to test associations with pathologic and molecular features. Of the analyzed images, 4186 cases included recurrence data, which was used to build the prognostic model.
The created AI model was applied to 2411 totally new cases from the colon cancer family registry (CCFR) for training purposes. On top of that, Dr. Pai preserved 1347 cases (external cohorts) to validate the model. “Building the AI model was actually not the most challenging part; collecting the data sets to validate the model was more challenging,” Dr. Pai explains.
Developing the QuantCRC-integrated stage II and III models
398 stage II mismatch repair proficient tumors were used to integrate AI into the ASCO stage II model, and 518 stage III tumors were used to integrate AI into the ASCO stage III model. The prognostic QuantCRC model categorized the stage II and III tumors into three groups: low risk, intermediate risk, and high risk. These risk groups were layered on top of the ASCO model, creating a more detailed risk scheme that Dr. Pai calls the QuantCRC-integrated scheme.
Read also: How did the Mayo Clinic choose a vendor for AI in pathology?
QuantCRC-integrated risk scheme: more powerful prediction of recurrence
A lot of work went into creating the AI model. Did it pay off? Did the QuantCRC-integrated risk scheme do a better job of risk-stratifying tumors?
Yes, it did.
The stage II QuantCRC-integrated risk scheme provides a more robust separation of low, intermediate, and high-risk cases. The AI model can potentially change who gets chemotherapy and improve admission to those who would most benefit from it.
While the stage III ASCO risk scheme only categorizes the tumor into low and high-risk groups, the new AI model identifies three groups. It shows an even higher risk group with a higher risk of recurrence compared to the ASCO scheme. This can make it easier to decide between three and six months of chemotherapy – reducing the total number of patients getting extensive chemotherapy but ensuring it is recommended for high-risk patients who can most benefit from it.
In the future, the 15 features chosen for QuantCRC could be used for multiple tasks. For example, when new therapies come up, they can be used to see if certain features predict the response to chemotherapy.
→ Watch the webinar recording: Using prognostic AI models in pathology: case colorectal cancer
→ Read more about the AI model: Aiforia® Colorectal Cancer QuantCRC
→ Listen to a podcast episode: How to approach colon cancer with supervised deep learning image analysis w/ Rish Pai, Mayo Clinic